

Coronavirus: Links, Discussion, Open Thread
Coronavirus: Links, Discussion, Open Thread
Will things get worse before they get better?
So far there have been three waves of coronavirus cases in the US. The first wave was the beginning, when it caught us unprepared. The second wave was in July, when we got sloppy and lifted lockdowns too soon. The third wave was November through January, because the coronavirus is seasonal and winter is its season (also probably the holidays). From Johns Hopkins CRC:
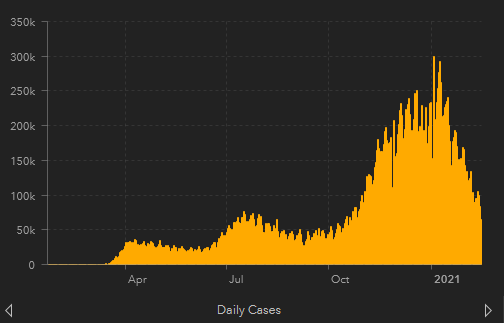
A fourth wave may hit in March, when the more contagious B117 strain from the UK takes over. Expect more shelter-in-place orders, school shutdowns, and a spike in cases at least the size of July's, maybe December's. That will last until May-ish, when the usual control system (more virus -> stricter lockdowns -> less virus -> looser lockdowns -> more virus) moves back into the "less virus" stage. Also coronavirus is seasonal and summer isn't its season. Also by that time a decent chunk of the population will be vaccinated. The worst consequences of the UK strain should burn themselves out by late spring.
Prediction: 75% chance that there will be a new wave peaking in March or April, with a peak at least half again as high as the preceding trough. [EDIT: some people link new studies saying the B117 strain is less virulent than previously believed, and the US has been getting much better at vaccination since I checked, probably my prediction above is too high and we should worry less about this]
We should also be concerned about a fifth wave (possibly overlapping with the fourth wave; they may not have obviously separate peaks). Virologists have identified two new strains, one in South Africa, one in Brazil, which probably have "immune escape" - the ability to infect people who have already gotten, recovered from, and developed antibodies to the original strain (or been vaccinated against it). Both strains already have a few cases in the US. It will take them a few months to spread to the point where they're relevant, but they should eventually be the majority of new cases.
Prediction: 66% chance that sometime this year, the South African and Brazilian strains - or other new strains with similar dynamics - will be a majority of coronavirus cases in the US.Some sources describe these strains as "vaccine resistant". This is a matter of degree. The UK strain is probably very slightly vaccine-resistant (most sources are describing it as not vaccine resistant, but if you look closely this is another "well we can't prove it is" situation, and the best point estimates suggest some tiny amount of extra resistance which probably doesn't make a big difference.). The South African strain is significantly vaccine resistant. The Brazilian strain is too new to know much about, but seems to be very similar to the South African strain and I would be surprised if its numbers differed very much.
In terms of preventing sympomatic infections, the best current data suggests that the Novavax vaccine is 96% effective against Coronavirus Classic, 86% effective against UK, and 60% effective against South Africa. AstraZeneca is something like 80% effective against Classic, 65% effective against UK, and the South African study was kind of bungled but our best guess is "seems pretty bad". Johnson and Johnson is 66-72%+ effective against Classic and 57% effective against South Africa. Pfizer/Moderna hasn't been tested against South Africa in real life yet, but lab studies suggest slightly decreased efficacy.
The good news is that vaccines which protect inconsistently against infection are probably still good at protecting against severe disease and death. For example, although the J&J vaccine is only 66-72% effective at preventing people from getting symptomatic disease, it's 85% effective at preventing severe disease, and (at least so far in studies) 100% effective at preventing deaths. In fact, most vaccine studies have shown 100% efficacy at preventing deaths. Probably some of this is that the trials are underpowered to detect rare outcomes, but the vaccines really do seem good at this, even with strains that have some level of vaccine resistance. Also, although I don't know of any studies investigating this, it makes sense to think that vaccinated people would also be less likely to transmit the virus to others if they do get it.
Prediction: 55% chance that later, when we have great evidence on this, we’ll find that P/M, Novavax, AZ, and J&J all cut deaths from all extant strains by at least four-fifths.When the fifth wave strikes in late spring/early summer, some of the population (~50%?) will be vaccinated, another part of the population (~25%?) will have had the disease already, and the rest (~25%?) will be completely vulnerable. The new strains will probably cause a limited number of mild cases among the vaccinated/resistant, and a larger number of more severe cases among the vulnerable. Either way, the presence of the larger vaccinated/resistant contingent could potentially make this less severe than previous waves. Also, we may have learned more about treating severe COVID (with eg ivermectin, fluvoxamine), which might further decrease deaths.
R in most US states right now is closely clustered around 1. Mutant strains are more contagious, enough to bring the R0 up to 1.5 or so. But having a lot of the population vaccinated will bring it back down again. Also, I'm acting like there's some complex-yet-illuminating calculation we can do here, but realistically none of this matters. It's not a coincidence that all US states are closely clustered around 1. It's the control system again - whenever things look good, we relax restrictions (both legally and in terms of personal behavior) until they look bad again, then backpedal and tighten restrictions. So we oscillate between like 0.8 and 1.2 (I made those numbers up, I don't know the real ones). If vaccines made R0 go to 0.5 or whatever, we would loosen some restrictions until it was back at 1 again. So unless we overwhelm the control system, R0 will hover around 1 in the summer too, and the only question is how strict our lockdowns will be.
In autumn, if we haven’t already vaccinated everyone there’s a risk things will get worse again because of the seasonal effect. Also, for all we know maybe the virus will have mutated even further and become even more vaccine resistant. Now what?
Vaccine companies say it should be pretty easy to create a vaccine targeted to the South African strain. Remember, it only took them two days to invent the original coronavirus vaccine. This one should be even easier, since we already know the principles involved. The vaccine is basically taking a part of the coronavirus' chemical code which functions as a "password" and telling it to the immune system so it can break its password and defeat it. The mutant coronaviruses haven't done anything fancy, they've just changed their password. The vaccine companies can plug in the new password to the vaccines they already have, and they'll work against the mutant strains.
But even if they have it tomorrow, that's...what? Another four months for studies, one month before the FDA is able to meet to discuss an approval (you can't rush meetings!), two months to ramp up production, and five months of Distribution Hell while we argue about who should be first in line and prosecute people for distributing vaccines too quickly. So maybe by this time next year you get a vaccine against the South African strain. And by that point the virus will have just changed its password again and we'll be right back where we started.
The problem is, all the virus has to do is change its chemical "password" - a simple one-step process. The people fighting the virus have to go through the entire FDA approval, production, and distribution pipeline each time - a seven million step process. This puts us at a bit of a handicap.
Best-case scenario, here's how we respond:
The FDA declares that all vaccine approvals it's already granted are extended to include minor updates to respond to new mutations, indefinitely. They agree that the general method is safe and effective, and so whenever the virus changes its password, the vaccine companies can create updated versions of the vaccines which include the virus' new password. Maybe they retest for safety (easy) but not efficacy (hard). Maybe this works for some of the vaccines involved but not others, I'm not sure.
Then they act as if they want vaccines to be produced. They subsidize all the existing companies and factories. They allow anybody to manufacture vaccines and charge market price for them, subject only to usual safety restrictions. If Amazon wants to get into the vaccine distribution business, for God's sake, let them. If that means some poor people can't afford vaccines, the government throws money at them until they can.
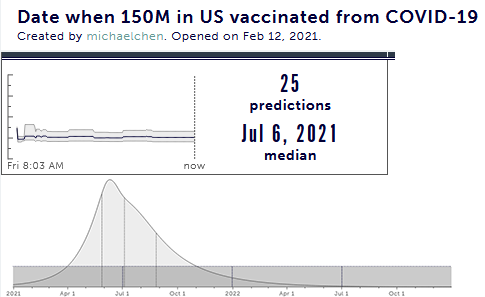
I don't think any aspect of coronavirus response so far could fairly be described as "best-case scenario". But if we manage to pull it together this time, I think we could bring the time from "discover new strain" to "vaccine for that strain is in your arm" from the current ~12 months down to ~2. Even granting it will take a few months to ramp up to this much better regulatory regime, that would be enough to give us a vaccine with full efficacy against the South African strain before it completely sweeps through the the US.
At that point - about six months from now - the real endgame starts.
Some number of people will have gotten vaccinated against coronavirus. Polls are kind of inconsistent about how many people plan to do this, but it looks like 66% is a good guess. Some additional number will have already had coronavirus. So at some point we get herd immunity to Classic, and at some slightly later point we get herd immunity to South Africa, even though it can potentially infect vaccinated people a little.
Then the virus mutates again. Mutation rate is a function of number of cases, so as number of cases goes down mutation rate should also go down, but number of cases probably isn't going down to zero in the US for a long time if ever, and parts of the Third World are going to take forever to be vaccinated, either for logistical or political reasons. We're not going to literally eradicate the coronavirus this year, and probably not this decade. So it will always have a chance to mutate and become more vaccine-resistant, and the new vaccine-resistant strains will give it more chance to transmit and therefore more chance to mutate, and so on.
Each new mutation is another 2-12 months of vaccine scramble. Also, although 66% of people are willing to get one vaccine, I think a lot fewer peopple are going to be willing to get a new vaccine every 2-12 months, especially if there's no guarantee it will end anything, and especially especially if lockdown is over and coronavirus has left the news cycle.
The most likely way this ends is that the coronavirus becomes another seasonal flu. Every year, the flu mutates a bit. Every year, we tell people to go in for their flu shots which make them immune to (our best guesses about) this year's flu. Every year, in the winter, flu sweeps across the world, a little slower in highly-vaccinated countries and a little faster in unvaccinated ones, and kills a six-digit number of people. Every year, this sucks, but at least in First World countries most of the elderly have been vaccinated and so it's less bad than it could be.
This is how I picture the coronavirus situation ending too. Enough people get vaccinated that it's no longer an abnormally dangerous pandemic. Each year, it mutates a little bit, and we change our vaccines a little bit. Unusually at-risk people and unusually-conscientious people get the vaccine; everyone else ignores it. Then we let it happen, mourn the dead, and go on.
Prediction: 60% chance that in 2022, public health officials recommend that you get “your yearly COVID shot”, even if you have previously been vaccinated against COVID(I want to make it clear I'm not saying COVID is currently "just the flu". It is currently much worse than the flu. Once everyone is vaccinated against several strains of it, the additional burden of a new strain might be no worse than the flu. Or it might be several times worse than the flu, but still on the same order of magnitude, to the point where it’s worth deploying the same intuitions to think about it. I doubt very much it will be as bad as it is now.)
[EDIT: Tomas Pueyo thinks this might not happen because the mutation rate is pretty low. But Trevor Bedford thinks the mutation rate might actually be pretty fast. Right now we’re not sure whether COVID is just picking the low-hanging fruit for good mutations or actually really good at mutating; depending on which of these is true we might or might not see the flu-like pattern.]
I don't usually think about this, but a biologist friend confirms: the number of diseases is increasing over time. More and more pathogens evolve to take advantage of human dominance of the planet. Cows and monkeys are out; humans are the Next Big Thing in the infection industry. Health care improves faster than diseases evolve, so on net fewer people die from infectious disease each year. But just because we're winning the race in general doesn't mean we win every leg. New diseases just occasionally get added to the world and stick around permanently. Fifty years ago nobody had to worry about AIDS; now lots of people do. The coronavirus will become a part of daily life, and it's going to suck.
I expect people to worry about this about as much as they worry about the flu now, ie not much. But I'm not sure exactly how it plays out. There will have to be some moment at which shelter-in-place restrictions loosen up and stay loose. I hope this will be as an adjustment to gradually increasing vaccination rates and gradually decreasing case numbers, and not as an unconditional surrender because we can't get our act together and the stress of new vaccine-resistant strains becomes too much.
On the opposite hand, some of my patients are anxious that lockdown will never end. Often these people are a bit paranoid or have a political axe to grind. But are they 100% definitely wrong? Some changes probably won't revert: at least some businesses have expressed some level of plan to go permanently work-from-home. I bet we'll pick up the Asian custom of wearing masks in crowded areas if we feel sick. Doordash-style food delivery companies were always going to grab market share; COVID just sped up the process - but it sped it up a lot, and it wouldn't surprise me if a lot of restaurants never re-opened, or only re-opened "in the cloud". I'm rooting for a permanent suspension of restrictions on telemedicine; now that everyone has seen it can be safe and effective, it would be perverse for the government to reinstitute all the roadblocks after things clear up.
Beyond that, we move into the really paranoid stuff. What if we never have rock concerts or music festivals again? What if places want you to wear masks forever, because there will always be a little bit of coronavirus or flu or common cold floating around? I think the chance of this is really low, less than 1%. But I hate to say 0%. Grade-school kids used to wander around town on their own or in bands of friends, playing games and exploring. Then there were various panics about child kidnappings and people insisted kids stay within their parents' sight at all times. Now crime is way down, people have stopped panicking about kidnapping, but they'll still call the police if they see an unattended kid because that just isn't done. There are whole countries whose cuisines are still built around weird decisions they made as part of World War II rationing. I really don't want this to happen, but I also didn't want normalized perma-surveillance after 9/11, which cured me of thinking anyone cared very much what I wanted about this kind of thing.
Prediction: 90% chance that on an average day in mid-2022, on an average street in the SF Bay Area, fewer than a tenth of people will be wearing face masks.I think we're far enough along now that the possible endings are scattered across a narrower region of probability space. Right now the best things governments can do is approve existing vaccines, work very quickly on a regulatory framework for constantly-changing vaccines, and start a flu-style program for ensuring a yearly coronavirus vaccine featuring up-and-coming mutant strains arrives at doctors' offices in time for the start of winter disease season. I’ve heard rumors that some officials are already thinking along these lines, which is heartening.
Prediction: 50% chance that sometime in 2021, the FDA grants a pharmaceutical company general approval for coronavirus vaccines which can adapt to changing virus strains without going through the entire FDA approval process again, and that whatever fast-track lane they get takes less than three months between creating the vaccine and it being approved for general use.This is the revival of the old Coronalinks / Open Thread, so feel free to use the comments for any coronavirus-related discussions you want to have.
Oh, and in case you’re one of the new readers I picked up this weekend and you don’t know how it works: I record all these predictions and grade how I did at the end of the year. You can see my past record here and by following the links at that post. If you disagree with me, consider telling me what confidence level you would assign to the statements I made, or making predictions of your own.
Coronavirus: Links, Discussion, Open Thread